Medicine and Health
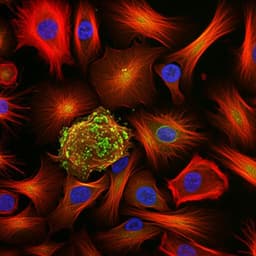
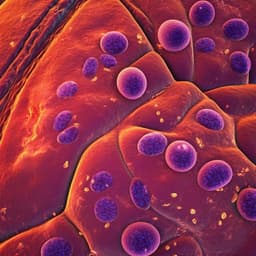
Single-cell sequencing of ascites fluid illustrates heterogeneity and therapy-induced evolution during gastric cancer peritoneal metastasis
X. Huang, M. Pang, et al.
This fascinating study delves into the complexities of peritoneal metastasis in gastric cancer, unveiling how certain immune cells evolve under therapy and their impact on prognosis. Conducted by a dedicated team of researchers, these insights shed light on the trajectories of cancer and immune cells during metastasis progression, promising innovative pathways for therapy-resistant cases.
Related Publications
Explore these studies to deepen your understanding of the subject.