Health and FitnessScientific Reports
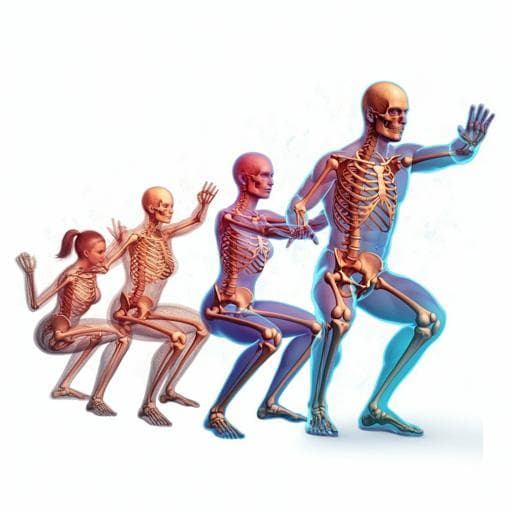
Sex-dependent differences in single-leg squat kinematics and their relationship to squat depth in physically active individuals
M. Zawadka, J. Smolka, et al.
This study reveals intriguing sex differences in single-leg squat kinematics among recreationally active individuals. Researchers found that joint angles and squat depth show distinct patterns between males and females, suggesting unique motor strategies during this exercise. This research was conducted by Magdalena Zawadka, Jakub Smolka, Maria Skublewska-Paszkowska, Edyta Lukasik, Aleksandra Bys, Grzegorz Zielinski, and Piotr Gawda.
Related Publications
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Medicine and Health
Diversity in a dish: Leveraging organoids to reflect genetic ancestry and sex differences in health and disease
F. E. A. Soussi, F. Piraino, et al.

Medicine and Health
Diversity in a dish: Leveraging organoids to reflect genetic ancestry and sex differences in health and disease
F. E. A. Soussi, F. Piraino, et al.
Medicine and Health
Sex differences in adipose insulin resistance are linked to obesity, lipolysis and insulin receptor substrate 1
P. Arner, N. Viguerie, et al.
Medicine and Health
Maternal high-fat diet programs white and brown adipose tissue lipidome and transcriptome in offspring in a sex- and tissue-dependent manner in mice
C. Savva, L. A. Helguero, et al.


