
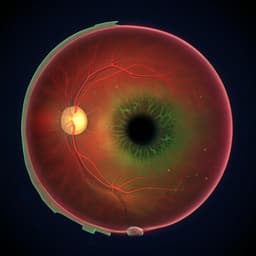
Autonomous artificial intelligence for diabetic eye disease increases access and health equity in underserved populations
J. J. Huang, R. Channa, et al.
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

What Is in There for Artificial Intelligence to Support Mental Health Care for Persons with Serious Mental Illness? Opportunities and Challenges
B. Wang, C. K. Grønvik, et al.

What Is in There for Artificial Intelligence to Support Mental Health Care for Persons with Serious Mental Illness? Opportunities and Challenges
B. Wang, C. K. Grønvik, et al.

The evolving field of digital mental health: current evidence and implementation issues for smartphone apps, generative artificial intelligence, and virtual reality
J. Torous, J. Linardon, et al.
Economic evaluation for medical artificial intelligence: accuracy vs. cost-effectiveness in a diabetic retinopathy screening case
Y. Wang, C. Liu, et al.


