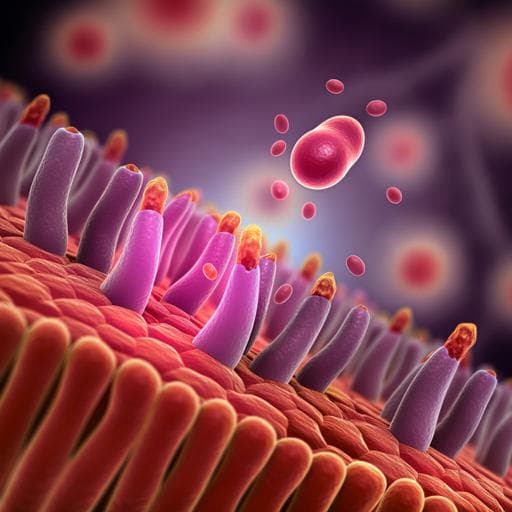
Nutritional deficiency in an intestine-on-a-chip recapitulates injury hallmarks associated with environmental enteric dysfunction
A. Bein, C. W. Fadel, et al.
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.
A pilot randomized controlled trial investigating the effects of an anti-inflammatory dietary pattern on disease activity, symptoms and microbiota profile in adults with inflammatory bowel disease
A. Marsh, V. Chachay, et al.
Joint association of sleep quality and physical activity with metabolic dysfunction-associated fatty liver disease: a population-based cross-sectional study in Western China
Y. Wang, Q. Zhao, et al.

Efficacy of an app-based multimodal lifestyle intervention on body weight in persons with obesity: results from a randomized controlled trial
K. Gemesi, S. Winkler, et al.

Academic burnout syndrome associated with anxiety, stress, depression, and quality of life in Peruvian dentistry students: an analysis using a multivariable regression model
J. Menacho-rivera, L. Castro-ramirez, et al.


