Medicine and HealthNature Communications
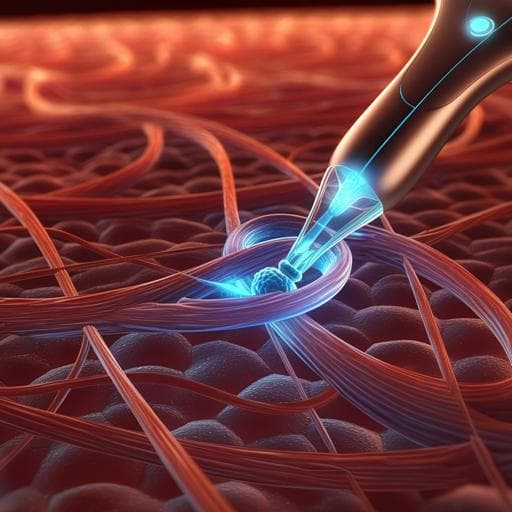
A wireless battery-free eye modulation patch for high myopia therapy
T. Zhong, H. Yi, et al.
Discover a groundbreaking approach to high myopia therapy with a wireless, battery-free eye modulation patch, powered by ultrasound. This innovative device dramatically reduces axial length and strengthens the sclera, offering hope for effective treatment. This exciting research was conducted by Tianyan Zhong, Hangjin Yi, Jiacheng Gou, Jie Li, Miao Liu, Xing Gao, Sizhu Chen, Hongye Guan, Shan Liang, Qianxiong He, Rui Lin, Zhihe Long, Yue Wang, Chuang Shi, Yang Zhan, Yan Zhang, Lili Xing, Jie Zhong, and Xinyu Xue.
Related Publications
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Medicine and Health
Wearable battery-free theranostic dental patch for wireless intraoral sensing and drug delivery
Z. Shi, Y. Lu, et al.
Medicine and Health
Fully implantable and battery-free wireless optoelectronic system for modulable cancer therapy and real-time monitoring
K. Kim, I. S. Min, et al.
Medicine and Health
Mesenchymal stem cell-derived exosomes as a promising cell-free therapy for knee osteoarthritis
D. Luo, H. Zhu, et al.
Medicine and Health
Fully implanted battery-free high power platform for chronic spinal and muscular functional electrical stimulation
A. Burton, Z. Wang, et al.


