Medicine and Healthnpj Systems Biology and Applications
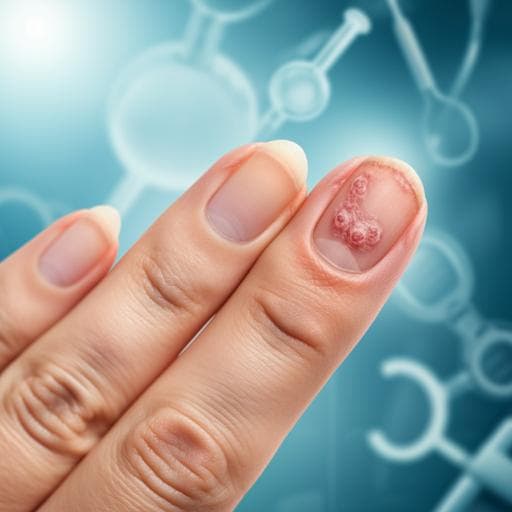
Reliable and easy-to-use calculating tool for the Nail Psoriasis Severity Index using deep learning
H. Horikawa, K. Tanese, et al.
Discover how the innovative 'NAPSI calculator' developed by Hiroto Horikawa and colleagues enhances nail psoriasis management by improving evaluation accuracy, potentially transforming clinical practices for patients impacted by this condition.
Related Publications
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Medicine and Health
Design and Analysis of a Deep Learning Ensemble Framework Model for the Detection of COVID-19 and Pneumonia Using Large-Scale CT Scan and X-ray Image Datasets
X. Xue, S. Chinnaperumal, et al.

Medicine and Health
Preferences for and intention to use an app for premenstrual mental health symptoms using the Health Behaviour Model (HBM)
E. L. Funnell, N. A. Martin-key, et al.

Computer Science
Using the interest theory of rights and Hohfeldian taxonomy to address a gap in machine learning methods for legal document analysis
A. Izzidien
Medicine and Health
Development and evaluation of deep learning algorithms for assessment of acute burns and the need for surgery
C. Boissin, L. Laflamme, et al.


