Medicine and HealthCommunications Medicine
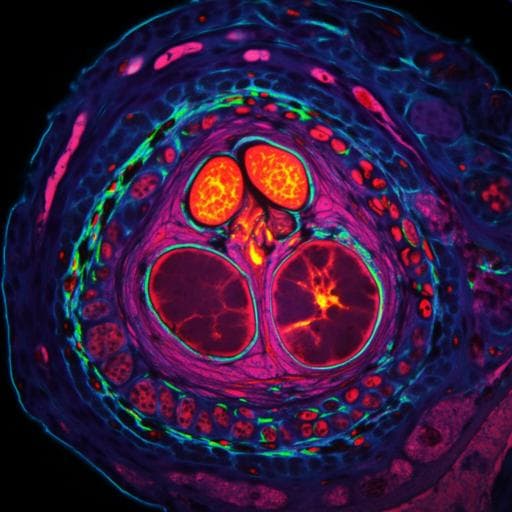
Predicting biochemical recurrence of prostate cancer with artificial intelligence
H. Pinckaers, J. V. Ipenburg, et al.
This groundbreaking study explores deep learning's ability to accurately predict biochemical recurrence of prostate cancer post-surgery. With promising results from 685 patients, these innovative findings by Hans Pinckaers and colleagues suggest that machine learning can uncover tissue patterns that might surpass traditional grading systems.
Related Publications
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Medicine and Health
Artificial intelligence unravels interpretable malignancy grades of prostate cancer on histology images
O. Eminaga, F. Saad, et al.

Medicine and Health
Diagnostic accuracy of point-of-care ultrasound with artificial intelligence-assisted assessment of left ventricular ejection fraction
P. Motazedian, J. A. Marbach, et al.
Medicine and Health
Effects of yoga in men with prostate cancer on quality of life and immune response: a pilot randomized controlled trial
D. Kaushik, P. K. Shah, et al.
Medicine and Health
Systematic review and meta-analysis of performance of wearable artificial intelligence in detecting and predicting depression
A. Abd-alrazaq, R. Alsaad, et al.


