Medicine and HealthScientific Reports
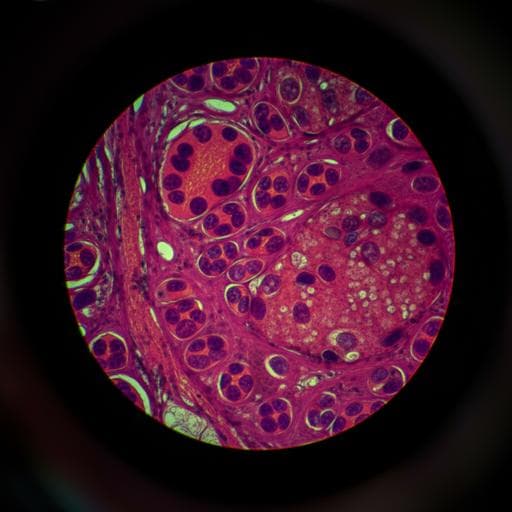
Effectiveness of transfer learning for enhancing tumor classification with a convolutional neural network on frozen sections
Y. Kim, S. Kim, et al.
Discover how researchers, including Young-Gon Kim and Sungchul Kim, are revolutionizing intraoperative metastasis confirmation using deep learning techniques. Their study highlights the potential of transfer learning from the CAMELYON16 dataset to significantly enhance tumor classification in frozen section biopsies, offering hope for improved surgical decision-making.
Related Publications
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Medicine and Health
Effectiveness of app-based cognitive behavioral therapy for insomnia on preventing major depressive disorder in youth with insomnia and subclinical depression: A randomized clinical trial
S. Chen, J. Que, et al.

Engineering and Technology
A convolutional neural network for defect classification in Bragg coherent X-ray diffraction
B. Lim, E. Bellec, et al.
Chemistry
A deep convolutional neural network for real-time full profile analysis of big powder diffraction data
H. Dong, K. T. Butler, et al.

Medicine and Health
Cumulative learning enables convolutional neural network representations for small mass spectrometry data classification
K. Seddiki, P. Saudemont, et al.


