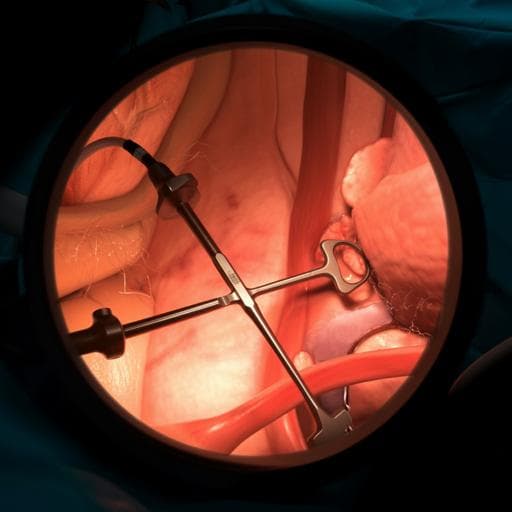
Development, deployment and scaling of operating room-ready artificial intelligence for real-time surgical decision support
S. Protserov, J. Hunter, et al.
Explore these studies to deepen your understanding
Adjacent work that informs or extends this paper's methodology and findings.

Development of prediction models for screening depression and anxiety using smartphone and wearable-based digital phenotyping: protocol for the Smartphone and Wearable Assessment for Real-Time Screening of Depression and Anxiety (SWARTS-DA) observational study in Korea
Y. Shin, A. Y. Kim, et al.

Artificial intelligence-based predictive maintenance, time-sensitive networking, and big data-driven algorithmic decision-making in the economics of Industrial Internet of Things
T. Kliestik, E. Nica, et al.
Development and evaluation of an artificial intelligence system for COVID-19 diagnosis
C. Jin, W. Chen, et al.
Nanoparticles and convergence of artificial intelligence for targeted drug delivery for cancer therapy: Current progress and challenges
R. P. Singh, A. Natarajan, et al.


